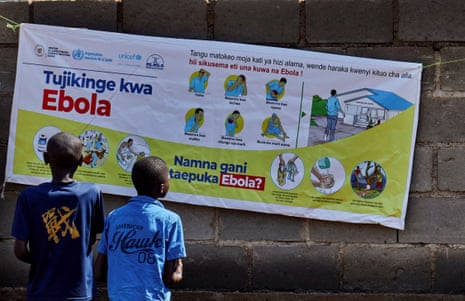
Ebola is spreading rapidly in parts of east Africa. The deadly disease, which kills around half of those it infects, is suspected to have claimed the lives of at least 240 people since the outbreak began in Ituri province in the Democratic Republic of the Congo earlier this month.
Public health officials are scrambling to contain the virus in one of the toughest environments: Ituri province, the centre of the crisis, is a mining hub where thousands of people work in close proximity every day, and a conflict zone, with ongoing fighting between rebel groups. Medical facilities are modest, while waves of displaced people are being forced into overcrowded camps to escape fighting, making it even harder to control transmission. The virus has already spread to other regions in eastern DRC and the Ugandan capital Kampala.
It is also the first major Ebola outbreak since the US, UK and other western countries made brutal cuts to humanitarian aid, which began with Donald Trump and Elon Musk’s gutting of USAID. The rapid response infrastructure from previous Ebola outbreaks has been stripped back so much of it is barely fit for purpose, hampering efforts to save lives, warn experts.
For today on First Edition, I spoke with Dr Papys Lame, the Ebola outbreak response coordinator in Ituri for the NGO Alima, and Selena Victor, senior director of policy and advocacy for Mercy Corps about efforts to contain the outbreak. But first, the headlines.
Five big stories
-
UK news | Britain risks a financial hit worth £125bn a year after a rise in the number of young people not in employment or education to more than 1 million.
-
US-Israel-Iran | Donald Trump has circulated a draft peace agreement for the war with Iran among allies including Israel as both sides try to prevent fresh breaches of the ceasefire escalating out of control.
-
UK politics | Andy Burnham has rolled back from his previous calls for ministers to scrap a restriction on immigrants claiming benefits as the Makerfield byelection places greater scrutiny on him.
-
Ukraine | A Russian drone that was part of an overnight attack on Ukraine crashed into an apartment building in eastern Romania, injuring two people, authorities said, in what an official statement condemned as an “irresponsible escalation” by Moscow.
-
Climate crisis | Abandoning net zero and drilling for more oil and gas would be a massive setback for the UK and would not help the economy, leading experts have said in response to Tony Blair.
In depth: ‘You must be brave if you work in this environment’
There is no current vaccine for Ebola. The virus, which is caught from wild animals and passed between humans through body fluids, was discovered in 1976 and is largely found in rainforest regions of western, central and eastern Africa. Between 2014 and 2016, the deadliest known outbreak killed 11,325 people in Guinea, Sierra Leone and Liberia. Frontline workers are desperately trying to prevent a repeat in eastern DRC and Uganda.
Lame says that Ebola was likely passing through the community for some time in and around Bunia, the capital of Ituri province, before the outbreak was formally declared on 15 May. Symptoms are similar to common illnesses like malaria and typhoid: fever, muscle pain, vomiting and diarrhoea. While Ebola is not spread as easily as a respiratory illness like Covid-19 or influenza, the lack of lab facilities for testing has made it hard to monitor. Many more cases are suspected than the official WHO figures, he says.
“We don’t have a specific treatment for Ebola right now but we can save people if they come very early. Then, their chance of being cured is higher. But if people come late, the case fatality rate is high,” says Lame, who is from Senegal. “Patients are afraid because they know that Ebola does not have a cure. Many have lost a member of their family or a colleague. And it also impacts frontline workers, too, who have lost colleagues.”
At least five doctors and nurses have died after treating patients at Bunia Evangelical medical centre, including 30-year-old Dr Vladimir Maduali who died on Sunday, and Dr Tibenderana Katho Blaise who died two days later. Other colleagues are believed to have contracted the virus.
“We have preventive measures that we are putting into place to protect our colleagues. They are working with some confidence because some have experienced previous Ebola outbreaks. You must be brave if you work in this environment,” says Lame.
Conspiracy abounds
Despite the immense bravery of medical staff, there is a fragile relationship with the local community, which is hampering the response. Some in Ituri province think that the virus does not exist or it has been brought in by humanitarian workers, fearing that they will die if they go to hospital, says Dr Lame.
There have also been attacks on healthcare facilities. The Ebola virus can spread from contact with cadavers, and authorities have implemented strict rules around burials which has sometimes angered families. In one case, a group of young men carried out an arson attack on an Ebola centre in the Rwampara region to try to retrieve a friend’s body.
Speaking about the attack on Alima facilities, Lame explains how the conditions around containment can exacerbate the sense of loss and anger: “The death of a young footballer from suspected Ebola shocked the community and his family. Young people came to ask for his body without treatment. Because it was a suspected Ebola death, we had to organise a safe burial so people got angry,” says Lame. “For us, this is not an attack against the organisation. It is anger and frustration against the loss of an important person in the community.”
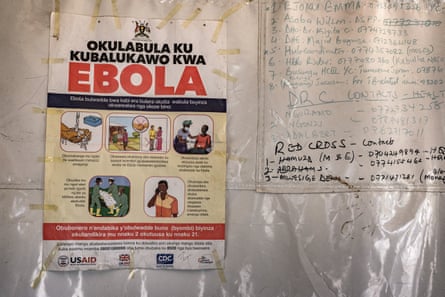
USAID cuts dismantled the system
Maintaining cooperation with the community is vital to ending the outbreak as quickly as possible, say public health officials. On Wednesday, World Health Organization chief, Tedros Adhanom Ghebreyesus, appealed for a ceasefire in Ituri between rebel groups to help contain the outbreak.
But the effort to end the Ebola outbreak will probably take several months. The 2014 Ebola outbreak in west Africa took more than two years to end, and there was a major international effort to protect people from the disease. Enormous western cuts to humanitarian aid appear to have made the response much slower this time. US foreign assistance to the DRC has fallen from $1.4bn in 2024 to $21m so far this year, with health officials warning that the US appears to be doing little to stop the outbreak this time.
“Ebola is one of those truly terrifying, upsetting, horrific things that does happen intermittently. Since the 2014 outbreak, we had gotten much better at identifying it and responding to the virus. There was a major effort to train local epidemiologists and health workers. The USAID cuts were obviously devastating. The system took a long time to build but didn’t take very long to dismantle,” says Selena Victor, senior director of policy and advocacy for Mercy Corps.
Some countries, including the US, are providing more funding to help. But the amount is dwarfed by the resources used to contain previous Ebola outbreaks – and officials are warning that basic PPE supplies were already a concern. The world must do all it can to make sure medical staff have the resources to respond this time, she said.
“I’m blown away by people’s willingness and commitment to help in these situations. Please, let’s not have a situation where they don’t have gloves, masks and gowns. The very least we can do is make sure that they have everything they need to stay safe,” she says.
A global problem
Last week, University of Oxford scientists said they are working on an Ebola vaccine that could be ready for clinical trials within two months, as part of the effort to contain the virus. The WHO is treating the outbreak as a public health emergency of international concern. But in the era of extreme political polarisation, governments are not responding as they have done to previous outbreaks.
The US has banned people from entering the country who have been in the DRC, South Sudan and Uganda in the previous 21 days. The Trump administration is also building a quarantine and treatment centre in Kenya for Americans affected by the Ebola outbreak, instead of bringing them home, attracting widespread criticism.
Lame said it was vital that his team get the resources they needed to help save lives – adding that more resources are still needed from abroad. “The community response against Ebola is critical, and we need many resources for this. International staff who can come and help with community engagement, human resources, logistics, water sanitation. Hopefully we will have enough to do our work.”
What else we’ve been reading
-
Argentina has a problematic self-image as “European” at the expense of African-Argentinian and Indigenous communities, as Tiago Rogero looks at what a recent spate of racist incidents says about race relations on the continent. Yassin El-Moudden, newsletters team
-
Laura Barton has a great interview with Paul McCartney about his early life and the inspiration for his new album. Patrick
-
Is Jamaica on the verge of becoming the region’s newest fossil-fuel producing state? Sarah Johnson takes stock of the debate triggered by news of a potential oil discovery. Yassin
-
Steven Morris has a brilliant report on volunteers rechalking the enormous Cerne Giant in Dorset this year. Patrick
-
Students in France are now able to say bon appétit over a three-course meal for no more than €1. Kim Willsher breaks bread with some of the beneficiaries of a student-led campaign that has borne fruit. Yassin
Sport
Tennis | Jannik Sinner’s bid for a maiden French Open title and career grand slam went up in smoke as he wilted in his second-round match against Juan Manuel Cerúndolo.
Cycling | Paul Magnier of Soudal Quick-Step completed a hat-trick of victories in this Giro d’Italia by winning a bunch sprint on stage 18 in Pieve di Soligo.
Athletics | Keely Hodgkinson has dangled the intriguing possibility that July’s London Diamond League meeting could be the day where she takes down Jarmila Kratochvilova’s 42-year-old 800m world record.
The front pages
“Labour plans welfare shake-up as scale of youth jobs crisis revealed”, is the Guardian’s front page today. The Times leads with “Burnham backs state control in blast at Blair” and the i Paper says “Burnham hits back at Blair and Starmer as he outlines plan to run Britain”.
The Telegraph says “Prostate screening set to be rationed” and the Mail, on the same topic, writes “Decision that will ‘condemn thousands’ to death”.
The FT’s splash is “Manifold clashed with BP’s company secretary before ousting over conduct”. The Express says “Jewish people don’t feel safe on British streets”. In the Mirror “Flags group ‘founder’ charged with murder” is the top story. The Sun goes with “It’s all kicking off” and finally Metro, on a drug gang who “loved the high life”, splashes “Behind spas!”.
Something for the weekend
Our critics’ roundup of the best things to watch, read, play and listen to right now
Film
Backrooms | ★★★★★
YouTuber Kane Parsons makes his feature directing debut with this icily brilliant and genuinely disturbing conceptual horror film based on his web series, and scripted by Will Soodik. There is something here of J-horror, the V/H/S found footage franchise, Dan Erickson’s Severance and Nathan Fielder’s The Rehearsal. It’s about people walled up in their own memories, imprisoned in endlessly remembered scenes from their past, or miserably perceived versions of their present existences in which they have become caricatures of themselves, gargoyle stars of their paralysed inner world of failure. Or perhaps the action of the film is not metaphorical in this or any other sense, and the “backrooms” of the title simply exist. Peter Bradshaw
Music
Iceage: For Love of Grace & the Hereafter | ★★★★★
Their sixth album, is billed as a return to punky first principles. It’s certainly less epic than its predecessor – but the barely contained chaos that Iceage once dealt in is conspicuously absent. Instead, the new album feels powerful, but streamlined in every sense, and the songwriting is extraordinarily tight and punchily melodic throughout. The songs have a sparkle to them: a curiously effective backing for Rønnenfelt’s lyrics, which still tend to the pugilistic, visceral and bleak, and make love sound like mortal combat. The result leaves you thinking that while the band’s constant development and diversity is striking, their consistency is more striking still. Alexis Petridis
TV
Spider-Noir | ★★★★☆
As the title suggests, Spider-Noir has been conceived as a homage to the hard-boiled films and fictions of the 1940s. The show is gloriously full of shadows and cigarette smoke, sassy secretaries and shady dames, as well as superheroes and supervillains. Plot twists are served up – and if none is brilliantly innovative, the whole is fast and fun enough to get away with it. Everything is shot with style and confidence, while the script contains just enough sharp dialogue and witty banter to keep it aligned with the templates of the past. And Nicolas Cage fans, of course, will have his turn as Ben Reilly to keep them going. Lucy Mangan
Theatre
Redcliffe, Southwark Playhouse Borough, London | ★★★★☆
Queer history is made up of bad news. The official documents record the raids, the arrests, the executions. The rest – all the raging love and snatches of joy – is largely left for us to imagine. In Jordan Luke Gage’s impressive Redcliffe, the writer-performer fills in the gaps of the lives of William Critchard and Richard Arnold, two men who collided in mid-18th-century Bristol. Inspired by true events romanticised into a musical, this is an open-hearted production. Kate Wyver
Today in Focus
Why are our homes and cities all so hot?
In the week when the hottest May days were recorded, the Guardian’s environment editor, Fiona Harvey, examines a new Climate Change Committee report on how the UK can better withstand extreme heat.
Cartoon of the day | Ben Jennings
The Upside
A bit of good news to remind you that the world’s not all bad
“That felt bonkers to me: they were creating the exact material we needed next to our site” says Joel de Mowbray, of the experience of watching trees felled near where he was working while he was having to source timber from miles away. He has now helped set up Tipping Point East, a hub set on a 20,000 sq metre industrial site in Newham, London, which promotes circular construction, where materials are reused instead of discarded. “We’re creating a regenerative supply chain for the city we love,” says De Mowbray. “Turning things that would otherwise go to waste into objects that have cultural potential”. The materials yard is full of neatly stacked glass panes, sinks and pipes that would otherwise have been thrown away which have now been certified to be re-used and donated to community builds or sold at very reasonable prices.
Sign up here for a weekly roundup of The Upside, sent to you every Sunday
Bored at work?
And finally, the Guardian’s puzzles are here to keep you entertained throughout the day. Until tomorrow.